77 yoF presented to the ED with left middle finger pain, swelling, and discoloration of ~1 week proximally (image 1).

Image 1: digit swelling and abscess
She was tachycardic and febrile on arrival. Physical exam revealed ¾ Kanavel signs (flexion at rest, pain with passive extension, fusiform swelling of the digit). Ultrasound was performed using a water bath (image 2).

Image 2: water bath technique
POCUS findings concerning for flexor tenosynovitis include a hypoechoic peritendunous effusion and a thickened synovial sheath that may be hyperemic.
Video 1/Image 3: shows fluid surrounding the flexor tendon in short axis.

Image 3: Short axis of flexor tendon with surrounding fluid
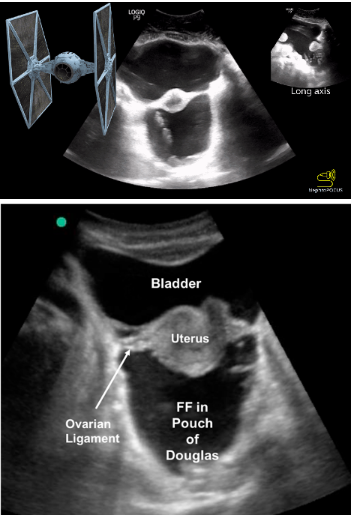
Video 2/Image 4: shows a long axis view of the finger with fluid in the pre-tendon area and surrounding edema.

Image 4: Long axis of flexor tendon with abscess/edema
Case conclusion: orthopedics was called and performed a bedside I&D. They were able to express “copious amounts of purulent fluid” but did not appreciate pus along the tendon sheath itself. The patient was admitted for IV abx and is getting daily wound checks by orthopedics.
Note: While the Kanavel signs and ultrasound are useful diagnostic aids, they are non-specific and should not be used as a rule-out test. Remember that many inflammatory processes will often create edema that appears hypoechoic on ultrasound.
Happy scanning!
- Ariella Cohen
References:
https://www.emdocs.net/ultrasound-probe-pocus-for-flexor-tenosynovitis/