Today’s pearl is in the form of a home-made infographic!
Here are a few key take-home points:
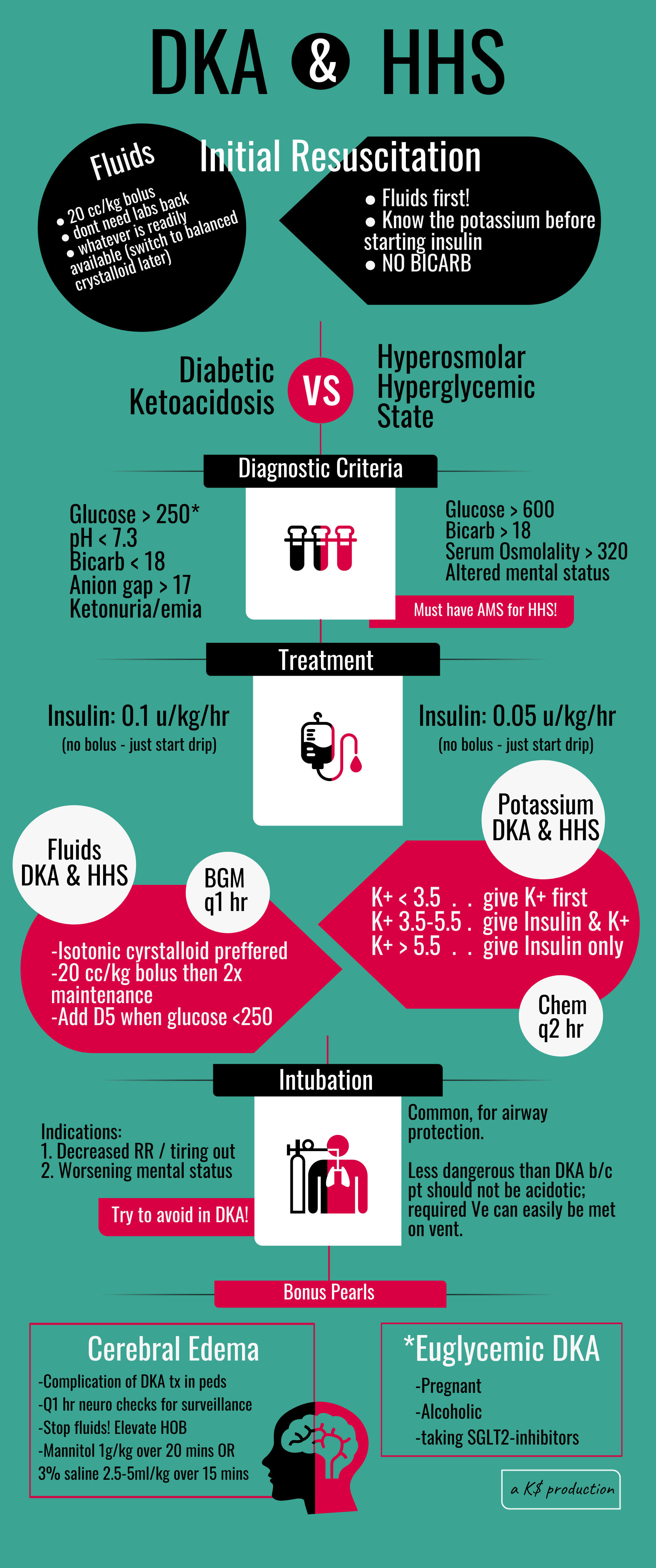
-Start fluid resuscitation ASAP (20cc/kg. you do not have to have any labs back.) Hang whatever fluid is convenient & change it later. The main concern with NS is that it will worsen acidosis if you give a ton of it. This is just the first liter, dont worry about hunting down your fancy plasmalyte right now.
-Do NOT start insulin w/out getting a K level – severe hypoglycemia can initiate arrhythmia & cardiac arrest
-Do NOT give Sodium bicarb even for a really low pH (6.7? I dont care. Didnt you read Duncan's pearls last month?!). The Bicarb is turned into CO2 which then has to be breathed off, and your DKA pt is already ventilating at maximum rate to correct the metabolic acidosis - you will just make this worse and make them tire out faster. (one exception being the hemodynamically unstable pt requiring pressors. Epi will not work with pH of 6.7, so you may consider bicarb).
-Euglycemic DKA may have glucose <250. This is seen in pregnant pts, alcoholics, and people taking SGLT2-inhibitors (drugs that end with -flozin) which block the absorption of glucose back into the blood stream at the kidneys.
-AMS is what differentiates HHS from just regular hyperglycemia (which usually comes w/dehydration as well, but that pt shouldn’t be altered).