QUESTIONS
EKG #1
36 year old, swole, healthy male, sharp diffuse anterior chest pain after pumping mad weights at the gym yesterday. He has a snake tattoo on his shoulder.
Like, what? Why?
How would you describe this EKG over the phone to a consultant?
What's the most likely EKG diagnosis? Anything else on your ddx?
Name two EKG findings that support your diagnosis.
Are you getting a troponin on this patient? If so, how many?
EKG #2
28 year old female, recent fever/cough, now with pleuritic/central/sharp chest pain. Kind of whiney. She’s on her phone.

1. What’s the most likely diagnosis?
2. Name two findings that support your diagnosis.
3. Is this EKG different from the previous? If so, how?
EKG #3
46 year old male with chest pain

1. What is the diagnosis? What about the EKG supports your diagnosis?
2. Is this EKG different from the previous two? If so, how?
ANSWERS
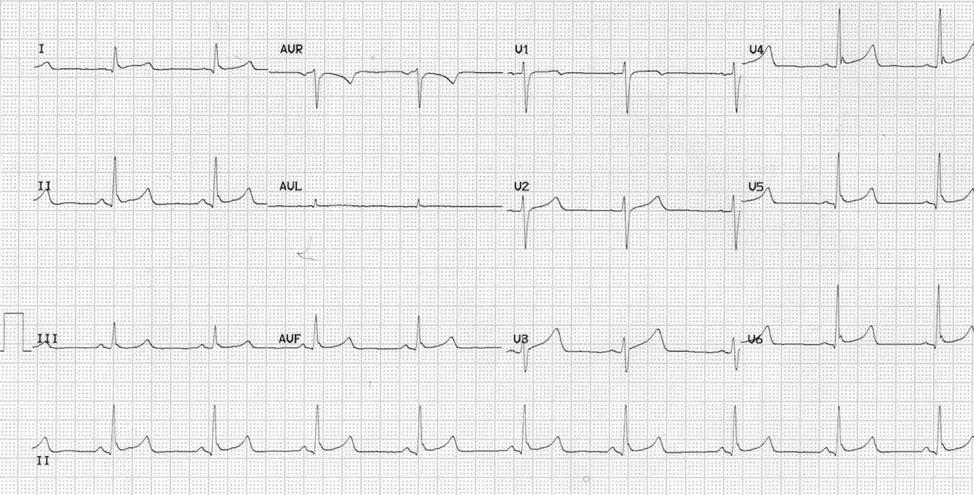
EKG #1
Benign Early Repolarization
· BER is a super common EKG pattern, so be familiar!
· Two main findings:

o Diffuse concave ST elevation, more-so in the precordial leads (usually < 2mm)
o Elevation & notching at the J-point.
§ Notching best seen in V4 – may look slurred in other leads
· Importantly, there are NO RECIPROCAL CHANGES
· Be suspicious of this diagnosis in patients over 50yo, consider ischemia
· With regards to the troponin, this is probably a style point, and I’m not sure there’s a right answer. Some attendings probably won’t get one. Most will just order one at the onset and call it a day. Some will argue that you can’t rule out ACS without serial troponins.
EKG #2
Pericarditis
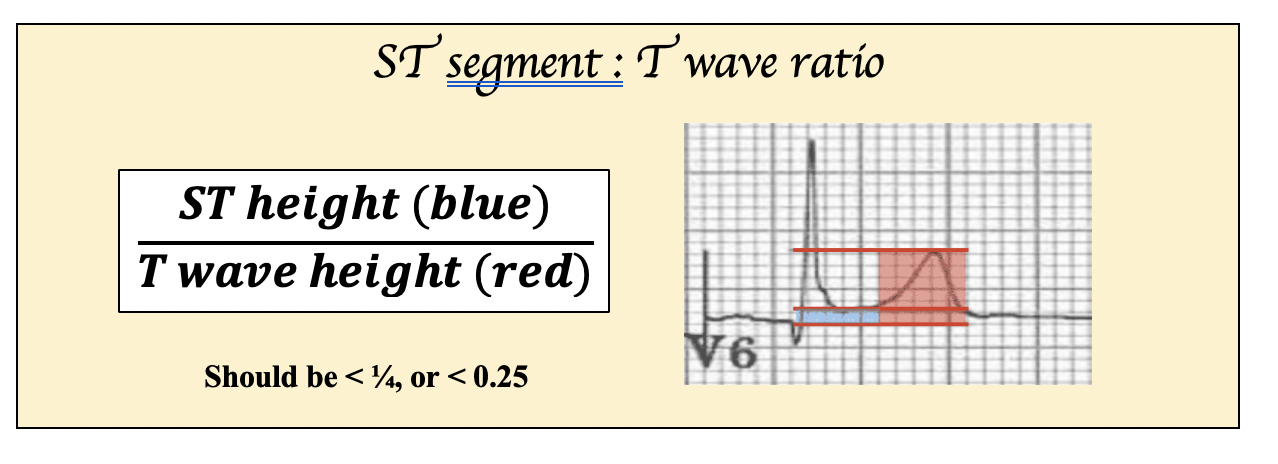
· Like BER, pericarditis also has diffuse concave ST elevation!
So how do we distinguish between BER and pericarditis??

EKG #3
Anterior STEMI
THIS IS AN IMPORTANT EKG. Our job isn’t to diagnose BER – it’s to see if our patient is having a heart attack.
Why is this an AMI and not benign early repolarization?
1. ST segments are nearly linear and lack the obvious concavity of the other EKGs
2. There is reciprocal change in lead III (look to inferior leads in anterior STEMI)
3. Leads V2-V4 have scary (pathologic) Q waves
4. There is poor R wave progression (there should be at least 3mm in V3 – here it’s 0mm)
Finally, for those of you who want to take it to the next level…

· This is actually an anterior MI, which is super frightening.
· It’s concave, there aren’t Q waves, there’s not reciprocal depressions (?III is inverted), though there is poor R wave progression and the T waves look big.
· There is a crazy formula you can use to distinguish BER from an AMI.
(1.062 x STE at 60 ms after the J-point in V3 in mm) + (0.052 x computerized QTc) - (0.151 x QRSV2) - (0.268 x R-wave Amplitude in V4 in mm)
· >18.2 is likely an LAD occlusion.
· More important than knowing this formula is knowing…
o Just because you don’t see a STEMI doesn’t mean they’re not infarcting
o If you’re suspicion is high enough, get a repeat EKG
RESOURCES FOR FURTHER READING:
Benign Early Repol - https://litfl.com/benign-early-repolarisation-ecg-library/
Pericarditis - https://litfl.com/pericarditis-ecg-library/
Anterior STEMI vs BER - http://www.emdocs.net/ber-vs-anterior-stemi/
Anterior STEMIs - https://litfl.com/anterior-myocardial-infarction-ecg-library/
For a super crazy next level anterior STEMI lesson…
https://hqmeded-ecg.blogspot.com/search/label/Examples%20of%20Formula%20Use--12%20of%20them